Psychiatric care lacking for institutionalised seniors
Don Weitz wears a T-shirt bluntly saying, “Fry rice - not brains.”
By David South
Today’s Seniors (Canada), November 1992
Seniors who live in nursing homes and homes for the aged are receiving an inadequate amount of psychiatric care, according to a study conducted by Toronto’s Baycrest Centre for Geriatric Care.
Dr. David Conn, director of psychiatry at Baycrest and an author of the report, says action must be taken to remedy this situation, since at least 80 per cent of elderly long-term care residents suffer from some form of mental disorder.
The issue of psychiatric care for seniors is complex. There are many, often strongly-held, opinions about the nature of this care and what measures will genuinely improve the mental well-being of seniors in institutions.
According to The Senior Citizens’ Consumer Alliance for Long-Care Reform, Ontario has the highest rate of institutionalisation of seniors in the world, with 7.5 per cent of seniors over the age of 65 and 15 per cent over 75 in institutions. The Alliance demanded in its reforms in Ontario that seniors’ mental health problems be taken more seriously and be included in any assessment for care.
Baycrest’s report surveyed 1,148 medical directors and nursing directors in over 500 nursing homes and homes for the aged across Ontario. The 601 who responded reported that 37 per cent of their residents received no psychiatric care, while only 12 per cent received more than five hours per month. The most common psychiatric problems under treatment were depression, agitation, wandering and physical aggression.
“Recognition of significant mental disorders in nursing homes is a recent phenomenon because geriatric psychiatry is a relatively new field,” says Dr. Conn. “The usual approach has been to reach for the prescription pad. We know now that antidepressants have been underused and tranquillizers overused.
“To deliver effective psychiatric care requires more than just psychiatrists - teams of psychiatric nurses can also be involved. Hopefully the staff of these institutions will become better educated as a result of this report.”
Dr. Kenneth Shulman, head of psychiatry at the Sunnybrook Health Sciences Centre, feels the worst neglect occurs in private rest homes.
“There is general lack of accountability when it comes to geriatric psychiatric services.” Schulman advocates a coordinated, comprehensive regional network of services.
Dr. Conn is sensitive to reports of sexual, physical and mental abuse of residents in some institutions. He says staff as well as residents of institutions can benefit from psychiatric consultations. “If more psychiatric consultants were available, the staff could also receive help in working out their problems,” he says. “Unfortunately the fee-for-service system doesn’t include paying for visiting staff.
“Being in an institution is not easy for anyone. It often means being apart from family, living with strangers, loss of freedom and having to live by the institution’s timetable.”
One of the most controversial of psychiatric treatments is electroconvulsive therapy (ECT). ECT involves placing electrodes on the sedated patient’s head and passing 100 to 175 volts of electricity into one of the lobes of the brain to induce grand mal seizure and coma.
Opponents of ECT say the procedure can cause memory loss and confusion, and in some cases proves fatal. A 1985 Ontario government task force report recommended against using ECT in certain cases: “For patients whose work requires a clear and precise memory, ECT is probably contraindicated.”
But many other sources say that while ECT has been abused in the past and, like many other medical procedures, may not be a pretty sight, it is sometimes effective in combating depression.
Dr. Conn confirms that the controversial procedure is still being used on seniors. “ECT is used on very depressed people,” he says. “It is a hospital-based service. The patient is admitted to a psychiatric unit of the hospital. We do it at Baycrest. It is only a last resort and has often been life-saving.”
Don Weitz, a senior citizen and spokesperson for Resistance Against Psychiatry, doesn’t mince words about what he says is the adverse effects of electroshock therapy and psychiatric practice in general. He wears a T-shirt bluntly saying, “Fry rice - not brains.”
“We have known about the adverse effects of shock for years,” says Weitz. “Research from the ‘40s and ‘50s was very clear that there was brain damage.
“What doctors mean by improvement is in fact post-injury euphoria - the brain will overcompensate with giddiness, and this only lasts for two to four weeks. Doctors seldom test people for more than two or three months afterwards.”
“What we know for sure is that within the institutions, they would rather give drugs or shock than talk to seniors. I think this should be called elder abuse - what else could it be? Is it such a mystery why people are depressed in institutions where they are abused? Psychiatrists have a vested interest in billing OHIP for pushing the button.”
But Dr. Shulman disagrees with blaming the atmosphere of institutions. “It is simplistic to think that the environment is responsible for aggressiveness or other problems,” he says. “These people are cognitively impaired - it could be medication-related or something else. These are complicated issues.”
For any nursing home workers who want further advice about psychiatry, Baycrest has produced a “Jargon-free” guide called Practical Psychiatry in the Nursing Home.


Private firms thrive as NDP ‘reinvents’ medicare
By David South
Today’s Seniors (Canada), August 1993
Many of today’s seniors fought for Canada’s internationally-admired public health system. But more and more people are becoming worried that the combination of health care reform, funding cutbacks and free trade is fuelling the growth of a second tier of private medical services serving the well off.
The provincial government sees things differently, arguing Ontarians no longer expect government to pay for everything and rather than eroding medicare, the NDP is reinventing it.
Whichever way one looks at it, private insurance companies, homecare providers, labs and other services designed to make money are becoming more and more involved in the health care business.
Operating in the territory outside the guidelines of the 1984 Canada Health Act - which sets out the principles of medicare for the federal government to enforce - the private sector has room to expand, at the same time as OHIP coverage is scaled back from more and more services.
Janet Maher, whose Ontario Health Coaltion (OHC) represents doctors, nurses and other health care workers, worries for the future of medicare.
“A number of things like accomodation services - laundry, food services - are in the grey area of the Canada Health Act,” says Maher. “So with all these fees that are being introduced, by the strict letter of the law, there is no way to stop them. But as far as we are concerned the spirit of the Act isn’t being observed.”
In its current reforms, the government of Ontario is emphasizing paramedical professions like midwives who fall outside the CHA and aren’t covered by OHIP. The turn to community-based services means that people have to rely more on services and providers that aren’t covered under the CHA.
Maher says privatizing accomodation services is a recent phenomenon, the result of hospitals finding creative ways to trim their budgets.
“It’s a new area that hospitals are taking bids on,” she says. “The other thing around the accomodation services is that because they are not categorized, strictly speaking, as health care services, none of this is exempted in the Free Trade Agreement from U.S. competition.”
A recent report by two British Columbia researchers tries to put together this complex puzzle. Jackie Henwood and Colleen Fuller of the 7,500-member Health Sciences Association of British Columbia recently charged that a combination of free trade and budget-slashing governments is eroding the universality of medicare and ushering in a two-tier system.
Fuller and Henwood identify the Free Trade Agreement as the culprit. While the health care industry created more jobs than any other sector of the Canadian economy between 1984 and 1991, they point out the job growth has been concentrated in the private sector since free trade was implemented in 1989. And they expect worse under the proposed North American Free Trade Agreement (NAFTA).
“NAFTA will accelerate trends towards a privatized, non-union and corporate-dominated system of health care in Canada.”
One provision of the Free Trade Agreement has also made it possible for U.S. companies to compete against Canadian firms in health care. Chapter 14, “health-care facilities management services”, allows wide-open competition.
Under NAFTA, provisions will bind all levels of government to consider for-profit health care companies on both sides of the border on equal footing with public providers when bidding for services, and entitles them to compensation if they can prove to an arbitration board they’ve been wronged.
“That represents a substantial encroachment on the democratic right of local, provincial and federal governments to make decisions,” says Cathleen Connors, who chairs the national wing of OHC, the Canadian Health Coalition.
It’s this plus health care cutbacks - federal and provincial - that’s resulting in service and job cuts and bed closures in the public sector and an increase in privatization, say Henwood and Fuller. These opportunities have not gone unnoticed by private companies south of the border.
One such company is American Medical Security Inc. (AMS) of Green Bay Wisconsin. After hiring Canadian pollsters Angus Reid to do a survey, AMS saw a profitable market in offering American hospital insurance to frustrated Canadians awaiting surgery. Sixteen per cent of those polled said they wanted this service; that was enough for AMS.
“One thing that comes across loud and clear is that Canadians for the most part are happy,” says spokesperson Carrie Galbraith. “They know they are taken care of during an emergency. But they are willing to pay a little extra if they need care.”
So far, AMS offers its plan to Ontario, B.C. and Manitoba, with Toronto its best market. Galbraith says plans are in the works to expand to all of Canada except the territories.
Unfortunately, like most private health plans, AMS cuts its losses by avoiding what Galbraith calls “adverse selection” - anybody with a known serious health problem need not apply.
Here in Ontario, private for-profit home care services take in close to half of all OHIP billings. Many clients pay out of their own pockets for additional services.
The Ontario health ministry doesn’t keep statistics on the extent of the private home health care sector, says spokesperson Layne Verbeek. But the Ontario Home Health Care Providers’ Association, a trade group, estimates private homecare companies now employ 20,000 and serve more than 100,000.
“It’s a market situation,” says Henwood. “If the services aren’t available to people within the public sector, they will go outside of it. We’ve seen this in other countries like England, where they had a public system and now have a parallel private system. If you erode a system enough that people get angry, they are going to start to look for alternatives, and the people with the greatest liberty are those with money.”
But in a recent interview, health minister Ruth Grier was adament this scenario wouldn’t be allowed to take place in Ontario. She strongly disagreed that medicare is being weakened due to recent changes, and said the government has actually “reaffirmed its commitment to medicare.”
 Austerity, Canada, Health, Magazine Stories 1990s, Media, Today's Seniors, Toronto
Austerity, Canada, Health, Magazine Stories 1990s, Media, Today's Seniors, Toronto Health care on the cutting block: Ministry hopes for efficiency with search and destroy tactics
By David South
Today’s Seniors (Canada), August 1993
It’s search and destroy time at Ontario’s ministry of health: search out savings and destroy inefficiency and waste. But many remain apprehensive that not all the cuts are going to be logical and fear the province’s health and well-being will be affected.
As part of the social contract deal, the Ontario Medical Association must find $20 million in cuts from the list of services covered by OHIP. The OMA and the provincial government are currently haggling over which procedures and examinations will be cut.
“We look at services that aren’t medically necessary,” says health ministry spokesperson Layne Verbeek. “Because we were wealthier in the past, we were able to cover some services. We aren’t in that position now. But I don’t see how eliminating medically unnecessary treatments will affect the population.”
The fallout of the Rae government’s attempts to reign in costs and recover lost revenues may take years to unfold, but it is already apparent that Ontarians will be paying more.
“Access to necessary treatment should not depend on a person’s ability to pay,” says health policy critic Carol Kushner. “What disturbs me about any delisting program is that virtually every medical service could be termed medially necessary. There are very few services that are an out-and-out waste of time.
“We often point to the fact that Ontario spends $200 million a year treating the common cold. Well, most of that is a waste of time. But delisting even that kind of service would be a detriment to the public’s health, because a small group of patients really do need to see a doctor when they have a cold.”
OMA spokesperson Jean Chow says it’s too early to pin down the exact cuts that will be made. “It’s a little premature to try and speculate what the final list will be.”
The newly-created Non-Tax Revenue Group is hard at work finding fees, fines and penalities the government can add or hike to boost revenue from this source from $5 billion to $10 billion a year.
The spring budget saw the first hit, with the addition of $240 million in non-tax revenue.
A radical reshaping of medicare is taking place. Private sector services - for which consumers pay directly or through insurance companies - now make up 34 per cent of Ontario’s health care funding, compared to 42 per cent in the United States, according to a recent study by the Canadian Medical Association.
Health minister Ruth Grier has also floated the idea of widespread hospital closures. Both the Toronto and Windsor district health councils (DHCs) are carrying out feasibility studies on “reconfiguration.” The ministry is remaining tight-lipped about which hospitals will get the chop.
“One suspects there’s room for efficiency - there are a lot of empty beds in a number of different places,” says ministry spokesperson Verbeek.
“All hospitals are being reviewed, with a view to closing one or two hospitals,” says health planner Lisa Paolatto, who is working on a feasibility study on “reconfiguration” for the Essex County District Health Council, along with Toronto’s DHC.
Closing hospitals could present a serious political hot potato for the government. In Britain, the Conservative government is still recovering from the bad feelings surrounding proposals to close world-renowned hospitals in the London area. The public feels great loyalty to local hospitals, a feeling that has been further fostered by hospital charities that raise millions a year from the communities’ good will.
“This is going to open up new discussions of money between doctors and patients,” says Kushner. “Seniors are a unique group in Canada because they remember what it was like before medicare - what it was like not to be able to pay for the doctor, to forgo treatment that they thought was necessary. They understand the financial hardship that could occur if they were unlucky enough to have a family member who needs expensive medical treatment.”
Feds call for AIDS, blood system inquiry: Some seniors infected
By David South
Today’s Seniors (Canada), July 1993
HIV-tainted blood transfusions given in the early 1980s have left some seniors with AIDS, but it is feared many are unaware of their HIV-positive status.
Between 1979 and 1985 - before testing of blood products for HIV became mandatory - 266 transfusion recipients and over 677 hemophiliacs are known to have been infected in Canada, according to the Centre for AIDS Statistics.
But the final numbers are unkown - estimates range from 400 to 1,000 cases of HIV transmission among the 1.5 million Canadians given blood products during this time.
This uncertainty is fueling public concern. With such a serious public health danger, many are shocked by the confusing messages being sent by governments, the Canadian Red Cross Society and hospitals.
But it took the report of an all-party Parliamentary subcommittee on health, released at the end of May, to shock the federal government into calling for a public inquiry into the blood system. The report is highly critical of the decision-making process involved in blood collection and distribution.
“We have members of our group who are seniors,” says Jerry Freise, spokesperson for advocacy organization HIV-BT (Blood Transfusion) Group, whose wife was infected with HIV due to a blood transfusion. “And many of them went for years being misdiagnosed and treated for something other than HIV. Others have gotten sick, and one died without knowing it because nobody told him.
“A classic case is Kenneth Pittman who was infected in 1984. The Red Cross found out in 1985 and they allegedly took two years to tell The Toronto Hospital. The hospital took two years to tell his doctor, and his doctor decided not to tell anybody.
Infected
“Another couple, a lady of 59 and a man of 64, called us April 1. She found she was infected, and the reason she took a test is because her husband turned out to be HIV-positive three weeks before a transfusion in 1983. He had gone for years without a diagnosis from doctors.”
This runs counter to the Red Cross’s story.
“Whenever a blood donor tests positive for HIV antibodies, we go back and trace the prior donations,” says spokesperson Angela Prokoptak at the Society’s national office. “The Red Cross supplies blood to hospitals, so we know which units went to which hospital. But the hospital must go through their records to find who they transfused.
“After identifying the recipient, the hospital contacts the recipient’s physician, and then they have them tested. There are of course limitations.
“Since 1987, the Red Cross has been advising people who may be concerned to consult their physician for counselling and advice.”
But subcommitte member Chris Axworthy, an NDP MP, found that hospitals and the Red Cross hesitated to notify former patients for fear of lawsuits. He says the federal government should show some leadership and stop passing the buck to other agencies and departments.
Only two hospitals in Ontario - Toronto’s Hospital for Sick Children and Princess Margaret Hospital - have tried systematically to contact former patients.
Ontario health ministry spokesperson Layne Verbeek says it is a laborious and costly task for hospitals to notify former patients. “We’ve always informed people if they are thought to be at risk, but many hospitals aren’t in the position to trace. If people are at risk or have doubts, they should be tested.”
Verbeek says recent media coverage has caused an increase in the number of people seeking HIV blood tests - requests for the test doubled after the Sick Kids hospital went public. The provincial government’s lab went from 700 tests per day to 1,300, but Verbeek says that has started to taper off.
The ministry of health is happy with the number of people coming forward to be tested, says Verbeek.
But Friese says the different players are more concerned about lawsuits than informing the public. He is especially upset at the Red Cross for not taking a leadership role in disseminating information.
“The Red Cross and the medical system have failed miserably to contact people. Even today they are reticent to tell people they were part of a risk group and should get treated.” Friese feels the various governments and the Red Cross are leaving the job of informing the public to his group and the Canadian Hemophiliacs Society.
Beat the drums
“It’s my job to beat the drums for the media while I’m dealing with my wife being infected? That’s my job, when these are the ministers of health?”, Friese says with anger.
The effect of AIDS on seniors isn’t new to US-based National Institute on Aging researcher Marcia Ory. She and colleagues helped sound the alarm back in 1989 with the book “AIDS In An Aging Society: What We Need To Know.” In the US, over 10 per cent of AIDS cases have occurred in people over 50.
“Surprisingly, people have ignored older people and the AIDS issue,” says Ory. “You had older people in hospitals who might have complained about fatigue which was thought to be age-related. Older people aren’t as likely to be diagnosed as early because of the assumption that they are not at risk from AIDS.
“We don’t want older people in general to be overly fearful, but we want them to acknowledge the possibility, and to engage in good preventative practices if they are at risk.”
Ron deBurger, director of AIDS prevention for the Canadian Public Health Association, would like assurances that the security of the blood supply has improved.
“The subcommittee came to the right conclusion asking for a public inquiry,” says deBurger. “I would hope the terms of reference are broad enough to take a look at the whole issue of the safety of the blood supply, not only in terms of what happened in the past, but, more importantly, what’s happening today.”
Other than hemophiliacs, who require large quantities of blood, deBurger believes anybody who received one transfusion has a small risk. “If you had blood once, I think the odds are pretty long that you are going to end up with tainted blood. But AIDS does take eight to 10 years to manifest itself, and we might still be picking up pieces for the next four to five years that we don’t know about yet.”
Friese recommends that anybody who received blood or blood products between 1979 and 1985 get an HIV test. If their doctor says it isn’t necessary, they should call the AIDS Hotline about anonymous testing.
Anybody who has tested positive for HIV and would like support and counselling can call Robert St-Pierre of the Canadian Hemophilia Society at 1-800-668-2686.
For information on anonymous testing call the Ontario government’s AIDS Hotline in Toronto at 416-392-2437. For support write HIV-BT Group, 257 Eglinton Avenue W., Suite 206, Toronto, Ont., M4R 1B1.
Austerity, Canada, Cities, Genetics, Health, Today's Seniors, Toronto, Virus Magazine Stories | Toronto 1992
By David South
Flare Magazine (Toronto, Canada) 1992
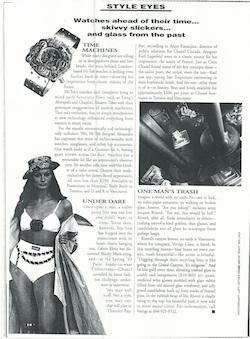
Time Machines
While many designers are telling us to don platform shoes and love beads, the man behind London-based Hi-Tek watches is looking even further back in time - drawing his inspiration from classic visions of the future.
Hi-Tek’s stainless steel timepieces bring to mind early futuristic films such as Lang’s Metropolis and Chaplin’s Modern Times with their grotesque exaggerations of modern machinery. That era’s confusion, fear, or simple wonderment at new technology influenced everything from toasters to steam trains.
For the equally economically and technologically turbulent ‘90s, Hi-Tek designer Alexander has captured this sense of techno-wonder with watches, sunglasses, and other hip accessories. One watch looks as if a Cuisinart hit it, leaving gears strewn across the face. Another has a retractable lid like an astronomer’s observatory. Yet another tells time with the blinker of a radar screen. Despite their made-exclusively-for-James-Bond appearance, all cost less than $190. Available at Possessions in Montreal, Body Body in Toronto, and D and R in Vancouver.
By David South
The Financial Post Magazine (Toronto, Canada), May 1992
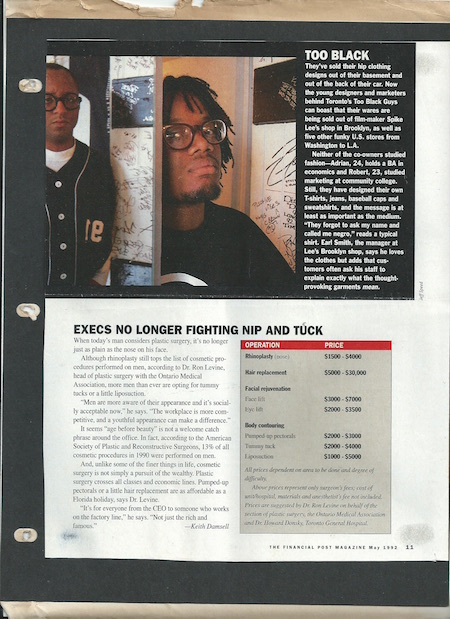
Too Black
They’ve sold their hip clothing designs out of their basement and out of the back of their car. Now the young designers and marketers behind Toronto’s Too Black Guys can boast that their wares are being sold out of film-maker Spike Lee’s shop in Brooklyn, as well as five other funky U.S. stores from Washington to L.A.
Neither of the co-owners studied fashion - Adrian, 24, holds a BA in economics and Robert, 23, studied marketing at community college. Still, they have designed their own T-shirts, jeans, baseball caps and sweatshirts, and the message is at least as important as the medium.
“They forgot to ask my name and called me negro,” reads a typical shirt. Earl Smith, the manager at Lee’s Brooklyn shop, says he loves the clothes but adds that customers often ask his staff to explain what the thought-provoking garments mean.
Other stories from the 1990s:
Aid Organization Gives Overseas Hungry Diet Food
Artists Fear Indifference From Megacity
The Big Dump: CP's New Operational Plan Leaves Critics with Questions Aplenty
Casino Calamity: One Gambling Guru Thinks The Province Is Going Too Far
Do TV Porn Channels Degrade and Humiliate?
The Ethics of Soup: Grading Supermarket Shelves - For Profit
False Data Makes Border Screening Corruptible
Freaky - The 70s Meant Something
Is the UK Rushing to Watch TV Porn?
Land of the Free, Home of the Bored
New Student Group Seeks 30 Percent Tuition Hike
Oasis Has Arrogance, A Pile of Attitude and the Best Album of 1994
Peaceniks Questioning Air-raid Strategy in Bosnia
Philippine Conference Tackles Asia's AIDS Crisis
Playboy ‘is not for sad and lonely single men’
Porn Again: More Ways to Get Off, But Should We Regulate the Sex Industry?
Somali Killings Reveal Ugly Side of Elite Regiment
Starting from Scratch: The Challenge of Transition
State of Decay: Haiti Turns to Free-market Economics and the UN to Save Itself
Study Says Jetliner Air Quality Poses Health Risks
Swing Shift: Sexual Liberation is Back in Style
Take Two Big Doses of Humanity and Call Me in the Morning
Taking Medicine to the People: Four Innovators In Community Health
Top Reporters Offer Military Media Handling Tips
Traffic Signs Bring Safety to the Streets
TV's Moral Guide in Question - Again
UK Laws on Satellite Porn Among Toughest in Europe
Undercurrents: A Cancellation at CBC TV Raises a Host of Issues for the Future
US Health Care Businesses Chasing Profits into Canada
Will the Megacity Mean Mega-privatization?
Will Niagara Falls Become the Northern Vegas?

This work is licensed under a
Creative Commons Attribution-Noncommercial-No Derivative Works 3.0 License.
Austerity, Canada, Cities, Digital, Health, Magazine Stories 1990s, Media, Now Magazine, Sarah Polley, The Toronto Star, This Magazine, Today's Seniors, Toronto, United Nations, University of Toronto, Youth 