Taking Medicine to the People: Four Innovators in Community Health
Preventing and treating illness at home or in small local clinics makes financial sense. It also makes patients a whole lot happier.
By David South
Canadian Living (Canada), January 1993
Your health is your wealth, my grandmother used to say. It certainly is our most valuable resource – and when its caretaker, universal health care, is under attack, people take notice
Provincial health ministries across Canada are scrambling to find new cost-efficient ways to deliver health care, and community health care is an increasingly talked-about option.
“Every royal commission has suggested we need to shift resources to community care and stop focusing on institutions,” says Carol Kushner, co-author, with Dr. Michael Rachlis, of Second Opinion (HarperCollins, 1990), a blockbuster book that challenges the way we approach health care in Canada. According to Rachlis, health care nationally cost more than $60 billion in 1992 and is primarily delivered through hospitals and doctors’ private practices. Yet 20 per cent of all patients in acute care hospitals don’t belong there, and about five per cent of hospital admissions for people over age 65 are the result of improper use of prescription drugs.
One study of the Toronto Health Unit found that as many as 50 per cent of seniors residing in nursing homes who were admitted to hospitals with pneumonia had contracted it through mouth infections. If they had received regular dental check-ups in the community or at institutions, these unnecessary and costly admissions could have been avoided.
Increasing numbers of people see community health care as the way of the future. In this model, health care providers – doctors, nurses and support staff – work as a team, and users of health care are involved in making important decisions. Community-based care supplements a medical approach to illness, with emphasis on social and environmental factors like work-related stress. Its advocates say community care can wean us off our addication to expensive hospitals (where one bed costs at least $100,000 a year), drugs and surgery – and make us all healthier.
“Fee for service” encourages doctors to see as many people as possible, emphasizing quantity over quality. In community health centres, doctors are put on a salary and encouraged to give as much attention as necessary to each patient. By simply spending more time with each patient, and by taking into account factors such as illiteracy and cultural differences, community clinics can cut down on misuse of medication.
Jane Underwood, director of public health nursing for the regional municipality of Hamilton-Wentworth in Ontario, says we have reached the limit of what hospitals can do to improve health. “Other factors are now more important than a strictly medical approach, which was the foundation of the old health care system. In 1974, a Health and Welfare paper urged a behavioral approach – stop smoking, get more exercise. Now we are moving to a socio-environmental approach, looking at poverty, social isolation, and unemployment, and their effects on health.”
“Community health care is inevitable because we can now do many procedures on an outpatient basis. With the new technology, all kinds of things can be done outside institutions,” says University of Toronto professor Raisa Deber, co-editor of the recently released book Restructuring Canada’s Health Services System (University of Toronto Press, 1992).
“Just as people can work out of their homes because of computers and faxes, technology can take medical care to the home.” This trend can already be seen in the treatment of cancer. Many patients now receive their chemotherapy at home, with the help of computerized IV pumps.”
If the debate over community health care often seems confusing, it may be because of the haphazard patchwork of programs across Canada. Quebec is the only province that took community health care seriously enough to set up clinics across the province in the 1970s and make those clinics an integral part of the provincial system. Elsewhere in Canada, programs sprang up in the ’60s and ’70s at the initiative of community activists but were met with indifference or hostility from government.
The challenge for community care advocates is to educate both the public and governments. Jane Underwood admits it will be a tough struggle. “Governments are beginning to understand, but the public still has reservations. They panic when there are fewer surgeries and feel that lots of high tech will provide a safety net for health. In fact, it is more scientific to probe for the true causes of illness and not think that just taking a pill will make us better.”
Four Innovators in Community Health
South Riverdale Community Health Centre, Toronto
This fully functioning health centre opened in 1976 in Riverdale, a multicultural and economically diverse neighborhood. The staff consists of doctors, nurses, chiropodists, social workers, health promoters and a nutritionist. Innovative in taking on economic concerns of the community, the centre has set up a community food market to provide cheap and healthful food and recently started workshops with business and community members to come up with strategies to recover jobs lost during the recession. "We consider ourselves part of a movement," says executive director Liz Feltes. And this is played out in projects with local groups and citizens on a variety of issues - from wife assault, drug abuse and sexually transmitted diseases, to medication literacy for seniors.
Victoria Health Project, Victoria
Originally started in 1988 to tackle the problem of poor communication between hospitals and community health providers, the project first targeted Victoria's large senior citizen population. Twelve programs were launched, including Wellness Centres, palliative support teams for patients dying at home and elderly outreach service focused on mental health. The project has been successful at getting local services to cooperate and eliminate duplication. "There are 500 different agencies for seniors in Victoria, so we linked up with them and increased cooperation," says Susan Lles, excutive coordinator of the project.
It was such a great success that the minister of health created the Capital Health Council to expand the program to the rest of the community. Now, for example, in hospital emergency rooms, quick response teams of nurses assess whether a patient would be better served by other services in the community or by being admitted to hospital.
Centres locaux de services communautaires (CLSC), across Quebec
Started in 1972 as part of province-wide health reforms, these comprehensive health centres now number 158, with more than 500 satellite offices all over Quebec. Every citizen is guaranteed access to a CLSC, even in remote areas. With five per cent of the provincial health budget, they are able to serve 41 pr cent of the population. They also involve the community through elected boards. "We think it is a unique model in that it integrates health and social services in the same place - both prevention and cure," says Maurice Payette, president of the federation of CLSCs. Because CLSCs are close to the community, governments, schools, community groups and other organizations have turned to them for advice during the last five years. In rural areas, CLSCs have been crucial in reducing the number of farm accidents.
Canadian Healthy Communities Project (CHCP), across Canada
Started in 1989, the program is aimed at municipalities and gets them to pledge that they will review all their actions with community health (including impact on the environment and economy) in mind. CHCP is part of an international movement linked with the World Health Organization's Healthy Cities movement. With more than 150 participating programs, it is an innovative attempt at getting the powers that be to plan for overall health. "We bring together community leaders to make a list of top 10 health problems and then decide what can be done with the existing budgets and staffing," says David Sherwood, project director. The city of Sherbrooke, Que., is a classic example. Facing reduced funds for road and sidewalk repairs, the city concentrated on repairs in neighborhoods with hig numbers of the disabled and elderly, thereby reducing the number of accidents. Unfortunately, funding was recently reduced dramatically by Health and Welfare Canada, but programs in Ontario, British Columbia and Quebec continue with the help of their own provincial government.
 "Taking Medicine to the People" was published by Canadian Living in 1993.
"Taking Medicine to the People" was published by Canadian Living in 1993.

This work is licensed under a
Creative Commons Attribution-Noncommercial-No Derivative Works 3.0 License.


 Canada, Canadian Living, Cities, Data, Health, University of Toronto
Canada, Canadian Living, Cities, Data, Health, University of Toronto Take two big doses of humanity and call me in the morning
By David South
The Toronto Star (Toronto, Canada), January 1, 1993
“Anybody going into medicine should read a whole bunch of good novels.” Dr. Alvin Newman isn’t kidding. The head of curriculum renewal at the largest English-speaking medical school in the world, the University of Toronto, feels strongly that doctors have been ill-prepared for their profession’s challenges.
How doctors become doctors is being hotly debated as Ontario’s five medical schools institute a potpourri of curriculum reforms. After a century of taking a back seat to scientific achievement, bedside manners and the art of medicine are in vogue again.
“Around the world, medical education is undergoing significant changes,” says Newman. “Medical schools must strike a balance between the incredible explosion of scientific knowledge and re-establish the role of the physician as wise counsel and empathic healer.”
It’s a role that many feel doctors have ignored. An American Medical Association poll, conducted between 1985 and 1988, found that fewer than 50 per cent of respondents said they thought doctors listened well and half believed doctors no longer care as much about patients as they used to.
In response to these criticisms, current reforms are shifting medical education away from reliance on the turn-of-the-century science-based approach, says Professor Jackie Duffin, a medical historian at Queen’s University who helped organize the new curriculum introduced there in 1991.
“In the old days doctors could probably make a diagnosis and tell people what was happening to them, but not do very much for them,” says Newman.
“Yet society had more trust and fondness for physicians than they do now. Much of the condemnation of the medical profession is because we have become the custodians of high-tech medicine.”
While the Ontario government embarks on the most sweeping reforms to health care since the 1966 introduction of comprehensive health insurance in Ontario and the founding of national medicare in 1968, many doctors feel their profession cannot afford to maintain the status quo.
The concensus at Ontario’s five medical schools – U of T, Queen’s, University of Western Ontario, University of Ottawa and McMaster University – has gelled around a belief that doctors need to be as comfortable dealing with people as they are with scientific medicine. To this end, revamped curricula supplement basic science and clinical medicine with emphasis on early exposure to patients, communication skills, psychological issues, medical ethics, medical literacy and health promotion.
These schools hope to produce new doctors to fit into a rapidly-changing health care system – one that many believe will rely far less on large hospitals.
Instead, many procedures will take place in the home or in the day clinics. Expanding community health care care centres will try to tackle extensive social and health problems. This preventive approach ot medical education was pioneered by Hamilton’s McMaster medical school.
Since its founding in 1967, McMaster has experimented with teaching methods that steer away from mass lectures to concentrate on the individual student. The evolution of McMaster’s curriculum has placed greater emphasis on communication skills, psychosocial aspects of medicine, community issues, and disease prevention and health promotion.
How do McMaster students rate against other medical students?
Last year they scored above the national average on licencing exams. A higher proportion of McMaster students enter research and academic medicine than their counterparts from other schools. One study comparing them to U of T suggested they were more motivated to be life-long learners.
Dr. Rosana Pellizzari practices the kind of medicine everyone is talking about these days. Working out of renovated church, Pellizzari’s practice at the Davenport/Perth Community Health Centre in westend Toronto serves a working class neighbourhood that has been home to generations of recent immigrants.
A member of the Medical Reform Group – which has long advocated significant reforms to health care – and trained at McMaster, Pellizzari can be seen to represent the doctor of the future: Sensitive, salaried and working in community health.
“McMaster’s curriculum attracts people with innovative ideas,” says Pellizzari, who was active in community health education before going to medical school. “It is a very supportive environment.
“I think the important question is: Who do we choose to be medical students? They should open up medical schools to those who know what it’s like to be a parent, a mother or disabled. Doctors should represent the population they serve. We are still getting mostly white, inexperienced young males as physicians. They aren’t going to practice the way that is necessary.”
In Ontario, many doctors see the 1986 doctors’ strike as a watershed for public opinion.
As a result of the negative fallout from the strike and perceived gap between physicians andhe public they serve, a five-year project entitled Educating Future Physicians for Ontario became a major advocate for reform.
Started in 1988, EFPO has examined fundamental issues in designing and implementing new medical school curricula. These issues include defining societal health care needs and expectations, faculty development and student evaluation. While each medical school has adapted reforms to its particular situation, EFPO hopes to prod further reforms.
“This is a unique venture in Canada, and could have implications far beyond Ontario if successful,” says Dr. William Seidelman, a key player in EFPO. “It captures the unique sense of the Canadian scene, and will build on the implied contact in the Canadian health system.”
Pellizzari sees the attitude of medical schools and teaching hospitals towards medical students as a significant factor in creating insensitive doctors. She recalls the high rate of suicide among medical students and the abusive work environment that forces doctors-in-training to work shifts unthinkable for other workers.
“The way we train doctors is inhumane,” she says. “We don’t expect other workers to put in 30-hour shifts. It creates in new physicians the attitude that they paid their dues and now society owes them.”
Many critics feel that changing training methods isn’t enough; the whole ethos and selection process must be changed. If doctors are to better serve the population, they must better reflect it.
“We are getting very close to gender equality and a laudable distribution of ethnic and racial backgrounds,” says Newman. “But students still come from a fairly narrow social spectrum, very middle class kids. Their exposure to the extremes of society, to poverty, to homelessness and related illnesses have been very limited.”
Pellizzari found how out-of-date the medical profession was in her first year. One teacher wanted her to work till 10 at night. When told that she needed 24 hours notice for a babysitter, the teacher shot back that motherhood and medicine don’t mix.
“I was a mother before I was a physician. When I get a call at night from a mother, I understand this. With 30 per cent of visits to doctors having no biological basis – like depression due to unemployment – you can’t do anything unless you have experienced life.
“If we don’t address this, you can design the best training in the world, but things won’t change.”
But Newman also feels many factors outside of medical school discourage a more diverse student body.
“To go through medical school in the United States requires large indebtedness. That’s not true in Canada. You can calculate what a year of medical school costs in terms of a finite number of CDs, a leather jacket and ghetto blaster. So something is dissuading people from pursuing this career, and it isn’t money.”
While there is a concensus among academics that medical schools haven’t prepared doctors well enough, there is little support for a dramatic change in selection criteria. “I can’t muster a lot of support from colleagues for serious changes,” says Newman.
Dr. Jock Murray, the former dean of Dalhousie medical school in Halifax, recently told an EFPO meeting he doesn’t see any significant changes ahead.
“Physicians have a reputation for being conservative and self-serving,” says Murray. “If reform is going to be successful we have to be clear that it is about what is good for the people.”
Pellizzari believes life experience and empathy with social circumstances just can’t be taught.
“I grew up in this neighbourhood. I understand their powerlessness, the conditions. Doctors have to see themselves as a member of a team of health professionals, not as the top of the social and medical totem pole.”
U of T’s experience is a classic example of the hurdles ahead. Newman admits it has come as a shock to students loaded with society’s ingrained expectations.
“They spend half a day a week in the community seing things like drug rehab clinics and community health centres. But being out in the community doesn’t make the students feel comfortable. Their image of what they are going to do involves big buildings, chrome and steel, scurrying personnel and banks of computers.”
 'Take two big doses of humanity and call me in the morning' was published in the Toronto Star in 1993.
'Take two big doses of humanity and call me in the morning' was published in the Toronto Star in 1993.
This work is licensed under a
Creative Commons Attribution-Noncommercial-No Derivative Works 3.0 License.
Starting from Scratch: The Challenge of Transition
By David South (Canada), UNV Information Officer, UNDP, Mongolia
UNV News #78 November 97
After seven years of transition to a market economy, Mongolia – a former satellite of the Soviet Union that has had a democratic government since 1992 – has been profoundly changed. Where it once had a rigid communist government and few contacts with the west, Mongolia has pursued rapid economic, political and social liberalisation. Mongolia has a small population – 2.3 million – spread out over a vast territory wedged between Russia and China.
Communication has in many ways deteriorated over the past seven years as the old communication networks from the communist era have not been fully replaced by the private sector. More and more it became apparent that government and the private sector were almost working in the dark in understanding how transition has affected Mongolians.
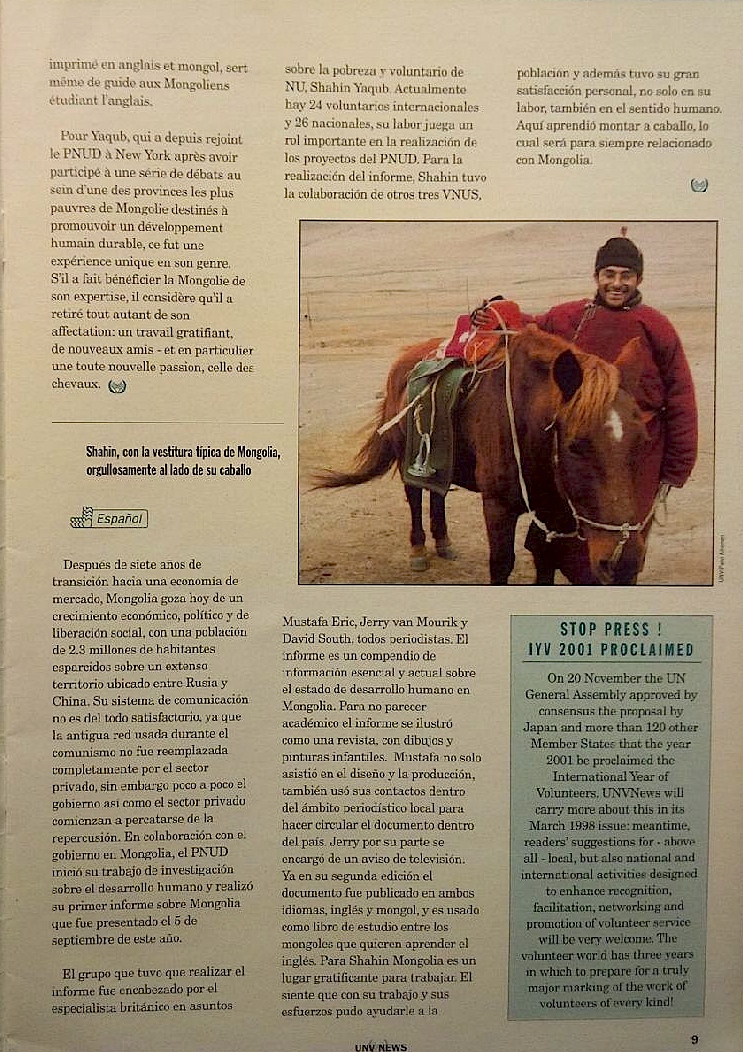
In partnership with the Mongolian government, UNDP initiated the researching of Mongolia’s first human development report back in the middle of 1996. It was launched on September 5 of this year, with UNVs playing a key role. To lead the team in producing the report, British poverty specialist and UNV Shahin Yaqub was brought in. Only 29-years-old – one of the youngest UNVs in Mongolia – Yaqub joined a rapidly expanding UNV presence in the country. There are now 24 international UNVs and 26 Mongolian UNVs deployed throughout the country in UNDP’s projects.
The thirst for expertise in Mongolia – a country undergoing the growing pains of transition to a market economy – has placed high demand on UNVs. UNVs occupy senior roles in all of UNDP’s projects.
The 1997 Mongolian Human Development Report is a prime example of the important goal of capacity building conducted by the UNDP. For Yaqub, the report’s principal author, it was like starting from scratch. A poverty research office had to be set up before the work could begin. A team of Mongolia’s top statistical researchers had to be trained in the latest methodologies for social research.
Yaqub was excited by the project. He said: ”There was no office when I first came. We had to organise the office to understand who does what and basically create the focal point for poverty analysis in Mongolia”.
Yaqub also had some of his basic assumptions tested. The small population of this country – only 2.3 million – had meant the previous communist regime was able to build up a large archive of statistics on the population. A good portion of the information was not up to international standards, but it potentially represented a wellspring of data to start from. “Mongolia is number-rich. To even have that kind of data is very rare for a developing country. But unfortunately we found all this information was stored on Russian mainframe computers that didn’t work anymore!”
During the actual production of the report, Yaqub was joined by three more UNVs: Mustafa Eric, a Turkish journalist working with the Press Institute of Mongolia, Jerry van Mourik, a Dutch journalist now working as the Support Officer to the United Nations Resident Co-ordinator, and UNDP Information Officer David South, a former journalist with the Financial Times in London, England.
The high-profile role played by media UNVs was crucial if the report was to not end up collecting dust on a government shelf. The report is a repository of essential and new information on the state of human development in Mongolia, including data showing rising poverty rates and serious threats to food security. Like all human development reports produced by UNDP, it was not meant to be a prescriptive tract, but a lubricant for a national debate on sustainable development in Mongolia. This altered the design and presentation of the report.
Instead of looking academic, the report took on the appearance of a magazine, from its cover to colourful children’s paintings inside. UNV Mustafa not only assisted with the report’s design and production, he also used his contacts in the Mongolian media to ensure the report was distributed across the country. UNV van Mourik assisted with publicity, including producing an emotionally-charged television commercial weaving together vignettes from Mongolia’s recent history to tell the story of human development.
Already in its second print run in both English and Mongolian, the report has been adopted as their study guide by Mongolians wanting to learn English.
“Mongolia is a rewarding place to work,” said Yaqub. “As a technical specialist and UNV, what you bring to the job is valued. I researched poverty for five years before coming to Mongolia and I felt I had something to contribute. But I also realised I had something to learn as well. You always have to keep in mind you are bringing your own baggage to the job – be it cultural, emotional or intellectual. Coming from an academic background, I was not afraid to be told I was wrong.”
Yaqub, who had worked in poverty analysis in the Philippines and Bangladesh before coming to Mongolia, will never forget the country that sparked his new passion: horses.
“You give up things as a volunteer – your time, your income, all the things you took for granted back home. But what you give up is compensated by rewarding work and good friends. When I learned to ride a horse, I can place it directly and clearly to Mongolia – that memory will always be with me.”
Just before Yaqub left Mongolia for work with UNDP in New York, he participated in a series of public debates in one of Mongolia’s poorest provinces, Khuvsgul aimag. The public debates are used to introduce the report to the grassroots while sparking discussion on sustainable human development.
 "Starting from scratch: The challenge of transition": UNV News, November 1997
"Starting from scratch: The challenge of transition": UNV News, November 1997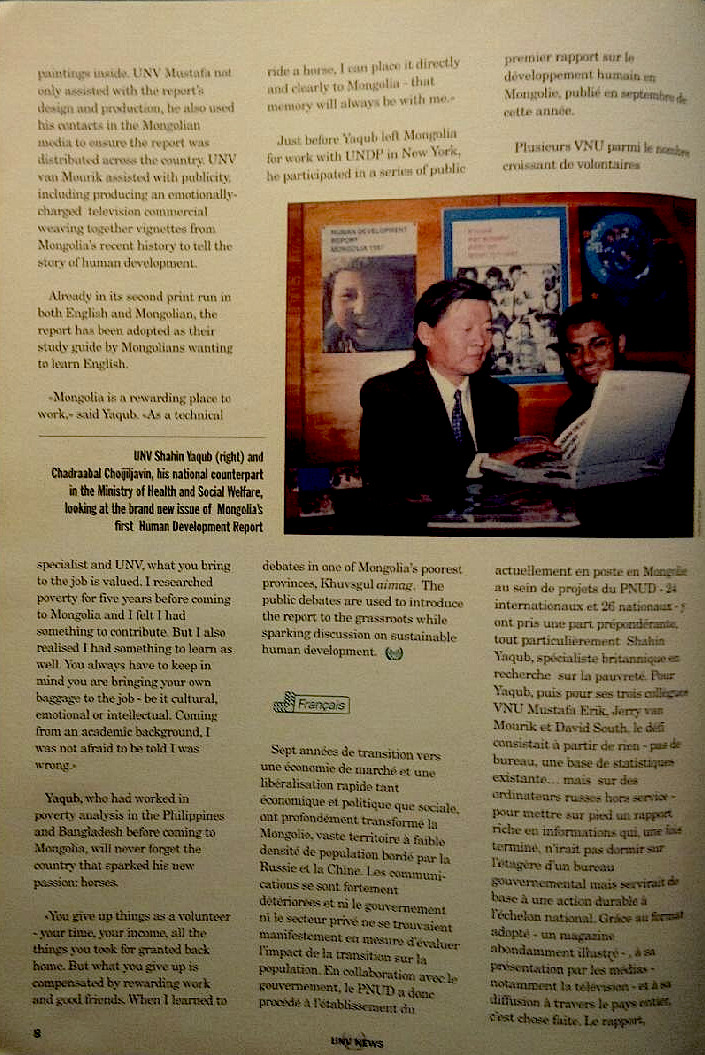
This work is licensed under a
Creative Commons Attribution-Noncommercial-No Derivative Works 3.0 License.
David South
 Buyng into capitalism: Mongolians' changing perceptions of capitalism in the transition years by Paula L. W. Sabloff (12 Oct 2020).
Buyng into capitalism: Mongolians' changing perceptions of capitalism in the transition years by Paula L. W. Sabloff (12 Oct 2020).
It was a pleasure to have the opportunity to comment on a draft of Buying into capitalism: Mongolians' changing perceptions of capitalism in the transition years by External Professor Emeritus Paula L. W. Sabloff from the Santa Fe Institute (12 Oct 2020: Central Asian Survey).
"A political anthropologist, she uses complex-systems tools to analyze three different databases: Mongolians’ changing ideas on democracy and capitalism, the emergence of early states all over the world, and 19-20th century Cozumel."
The Santa Fe Institute "is the world's leading research center for complex systems science."
Agenda 21, Austerity, Cities, Data, David South Consulting, Digital, ICT4D, Internet, Magazine Stories 1990s, Northeast Asia, Poor, Shock Therapy, Solutions, Strategy, Trade, UN Innovator Stories, UNDP, UNDP Innovator Stories, UNDP Mongolia, UNV News, United Nations, Women, Youth Study says jetliner air quality poses health risks: CUPE takes on airline industry with findings of survey
By David South
Now Magazine (Toronto, Canada), March 11-17, 1993
Canada’s troubled airline industry is about to face some more turbulence, as the union representing more than 6,000 flight attendents presses its concern that many of its members’ health problems are related to poor air quality in jets.
The Canadian Union of Public Employees (CUPE) says its locals have compiled data that paints a fairly stale profile of in-flight air quality and its relationship to altitude, passenger load and length of flight. As part of the survey, the union recorded flight crews’ complaints of chest pains and lack of oxygen, as well as other work-related problems like back injuries, hearing loss and high incidence of colds and flu.
Of more interest to frequent fliers might be the opinion of some experts that even the more common jet lag may be caused by excess carbon dioxide, ozone and radiation. More than half the air in many aircraft is recirculated, “stale” air that is high in carbon dioxide and may be carrying bacteria and viruses, according to some experts.
CUPE health and safety chair Tracy Angles says the union now has enough evidence to at least pressure the carriers to undertake more comprehensive air quality studies. CUPE represents workers at Air Canada, Canadian, Nationair, Air Transat and some smaller feeder carriers.
While the union’s study is the first of its kind in Canada, a survey by the US department of industrial relations found, among other things, that flight attendents had 20 times the expected frequency of respiratory illness.
Flying mines
“Flight attendants have been equated with coal miners in terms of the bad air they have to breathe,” says Angles. “But this is not something the companies want to study.”
However, spokespeople for Air Canada and Canadian Airlines say they have not heard of such health problems. Jerry Goodrich of Canadian simply says, “It’s not an issue.”
However, while earlier-model jets supplied the cabin with 100 per cent fresh air, increasing fuel costs led to some modification. Modern jets mix fresh air – expensive to produce – with stale air from inside the cabin, which is passed through filters. The percentage of recirculated air in some aircraft, such as the popular Boeing 747-400, could be as high as 52 per cent, Boeing’s figures show.
Boeing’s Tom Cole says air circulation in Boeing’s jets is better than in an average office building, and that the passengers are “washed” with air to eliminate carbon dioxide and other hazards.
Critics like Georgia doctor William Campbell Douglass, publisher of the health newsletter Second Opinion, charge that the high rates of recirculated air, and the reliance on passengers’ own breath and perspiration to humidify the dry air, provide a perfect environment for bacteria and viruses. Douglass even speculates that planes could transmit serious diseases like tuberculosis. He suggests jet leg could be “nothing more than CO2 intoxification and oxygen starvation.”
“There is no doubt if you are in a confined space, you are at greater risk,” says University of Toronto microbiologist Eleanor Fish. “Aircraft filter systems aren’t sophisticated enough to filter out all the bacteria and viruses. But I’d be hard pressed to believe that you are at greater risk traveling on airplanes than on elevators.”
It is difficult for public health authorities to pin down the health risks of airplane travel because passengers disperse immediately after a flight. However, medical journals have documented two cases where virus transmission could be established because the passengers were easily traceable.
In 1977, 38 of the 54 passengers on a plane grounded in Alaska for four and a half hours came down with the same strain of flu.
“We consistently hear complaints about certain aircraft,” says Angles. “The Airbus320 is one of the worst” Angles says many airlines exacerbate the problem by over-crowding planes and flying them longer and farther than they were designed for.
Cut corners
“With deregulation, they have more people in there than was ever planned on. Nationair is a good example. A normal class Air Canada 747 carries about 420 people. In the all-economy configuration the load is upwards of 496.”
Angles also says airlines have been known to cut corners by turning down air flow to save money. In their 1990 book The Aircraft Cabin: Managing the Human Factors, Mary and Elwin Edwards cite a study indicating that 1 per cent saving on a fuel bill can be achieved by reducing the ventilation rate in a McDonnel-Douglas DC-10.
 "Study says jetliner air quality poses health risks": Now Magazine, March 1993.
"Study says jetliner air quality poses health risks": Now Magazine, March 1993.
 The Google Snippet for the story. According to Neil Patel, "99.58% of featured snippet pages already rank in the top 10 SERPs in Google for a particular search query."
The Google Snippet for the story. According to Neil Patel, "99.58% of featured snippet pages already rank in the top 10 SERPs in Google for a particular search query."
More resources:
Jetliner Cabins Are Quickly Cleared of Virus, Pentagon Says
"Particles the size of the new coronavirus are quickly purged from a commercial aircraft cabin, according to a U.S. Defense Department study touted by United Airlines Holdings Inc. in its effort to reassure wary travelers.
Filtration systems and rapid air-exchange rates mean that only about 0.003% of infected particles entered a masked passenger’s breathing zone, said the report, released Thursday."
Aircraft Air Quality – Protecting Against Contaminants, Association of Flight Attendants
"On October 5, 2018, a 5-year FAA bill became law. Included in the bill is a study on technologies to combat contaminated bleed air. This is significant progress!"
'Contaminated air' on planes linked to health problems, 21 June 2017
Influenza Air Transmission, Influenza A (H1N1) Blog, September 28, 2009
"What does this tell us? Aerosols, very small particles of saliva containing the virus we exhale when we sneeze or even when we breathe if we have the flu, probably have an important role in the transmission of influenza. In addition to that we have public transportation, with a great number of people circulating in a place that may be closed and badly ventilated at times and we may have a notion of the importance of public campaigns that promote education and awareness of contaminated people to avoid leaving their homes when they have the flu and that they cover their mouth and nose with a disposable tissue when they sneeze and discard it right after that."
"A Jet airliner with 54 persons aboard was delayed on the ground for three hours because of engine failure during a takeoff attempt. Most passengers stayed on the airplane during the delay. Within 72 hours, 72 per cent of the passengers became III with symptoms of cough, fever, fatigue, headache, sore throat and myalgia. One passenger, the apparent Index case, was III on the airplane, and the clinical attack rate among the others varied with the amount of time spent aboard. Virus antigenlcally similar to A/Texas/1/ (H3N2) was Isolated from 8 of 31 passengers cultured, and 20 of 22 ill persons tested had serologic evidence of infection with this virus. The airplane ventilation system was inoperative during the delay and this may account for the high attack rate."
The Airliner Cabin Environment and the Health of Passengers and Crew.
"At the end of its review of health data in the 1986 report The Airliner Cabin Environment: Air Quality and Safety, the National Research Council (NRC) committee concluded that “available information on the health of crews and passengers stems largely from ad hoc epidemiologic studies or case reports of specific health outcomes [and] conclusions that can be drawn from the available data are limited to a great extent by self-selection…and lack of exposure information” (NRC 1986). This chapter reviews data on possible health effects of exposure to aircraft cabin air that have emerged since the 1986 report and the emergence of data resources (e.g., surveillance systems) and studies that have particular relevance for the evaluation of potential health effects related to aircraft cabin air quality. Selected earlier sources are also reviewed. The decision to ban tobacco-smoking on domestic airline flights in 1987 and on flights into and out of the United States in 1999 reduces the relevance of some studies of exposures and reported signs and symptoms that clearly could have been related to the products of tobacco smoke."
This work is licensed under a
Creative Commons Attribution-Noncommercial-No Derivative Works 3.0 License.
“Pocket-Friendly” Solution to Help Farmers Go Organic

Interest in organic food and farming is high, and organics have become a growing global industry. The worldwide market for organic food grew by more than 25 per cent between 2008 and 2011, to US $63 billion, according to pro-organic group the Soil Association. That is an impressive accomplishment given the backdrop of the global economic crisis, and evidence that people value quality food, even in tough times.
One Kenyan company is hoping to help farmers benefit from this global surge in interest in organic food. The company is selling a healthy alternative to chemical fertilizers and is hoping it will soon be able to source its products in Kenya, too.
BioDeposit (http://biodeposit.lv/index.php?page=elixir-3) sells soil conditioner and natural fertilizer made from two ingredients: peat found in marshlands and silt dredged up from lakes, which is called sapropel (http://en.wikipedia.org/wiki/Sapropel). This naturally occurring resource is rich in all the elements required for abundant crops and has the added benefit of not poisoning the soil and water table when used on farmer’s fields.
It is sold as a solution to the multiple pressures hitting farmers, from chaotic weather patterns to soil damage and decreasing yields. It offers a way to boost farm productivity without damaging the soil in the long term.
In 2011 the amount of farmland that was organic reached 37.2 million hectares in 162 countries – but this is still just 0.86 per cent of the world’s agricultural land (Research Institute of Organic Agriculture and International Federation of Organic Agriculture Movements). If BioDeposit has its way, Kenyan farmers could help to grow the number of hectares being farmed organically.
Presenting the solution in October 2013 at the Global South-South Development Expo (southsouthexpo.org) at the headquarters of the UN’s Environment Programme (UNEP) in Nairobi, Kenya, BioDeposit communications and media chief Nelly Makokha (http://ke.linkedin.com/pub/nelly-makokha/29/a08/634), explained that the company is hoping to bring the technology behind BioDeposit to Kenya, if they can get permission.
At present, the source materials for the products are dredged from lakes in Latvia in Eastern Europe. Because of the political structures of Kenya, it means a long political process is ahead to gain permission to dredge any of the country’s lakes. BioDeposit’s Latvian scientists conducted research on the potential for Lake Naivasha (http://en.wikipedia.org/wiki/Lake_Naivasha) in the Rift Valley and claim it has enough deposits to provide Kenya’s farmers with organic fertilizer for the next 200 years.
“If the government agrees, the fertilizer is basically cheaper than any other fertilizer the farmer [will] have ever used in a long time,” said Makokha. “It will be pocket-friendly for them. As they earn more money from the more yields, they are spending less on the fertilizer.
“Our slogan is ‘smart agriculture for health and wealth’ – health in terms of you become organically grown, and if you are looking for organic certification, we will organize that for the certifiers. Right now most countries are looking for organic food and cannot find it.
“So when you become organic that means you earn more money on your products so it means you are healthy and you are wealthy!”
The fertilizer comes in 12 milliliter packets that cost 200 Kenyan shillings (US $2.30). A farmer would need two packets for each quarter acre of farmland.
Based on a Russian discovery from the early 20th century, BioDeposit draws on naturally occurring resources.
Its products include BioDeposit Agro, described as a “biologically active soil conditioner,” and BioDeposit Elixir, described as a “humic plant growth stimulator.” The Elixir is a “sustainable, water-soluble” concentrate made from peat and can be used to soak seeds prior to planting, increasing the germination cycle. For the farmer, it means more seedlings in a shorter time. It also can be poured on compost piles to boost humic content to speed compost decay. Peat is formed from above-ground marsh plants, either on the surface or under a layer of water.
BioDeposit Agro is made from sapropel from the sediment at the bottom of freshwater lakes. It is a renewable, naturally-occurring resource as it has been formed from the accumulated settling of plants such as reeds, algae, trees, grasses and animals over time as they decay.
Unlike other chemical fertilizers, using the BioDeposit product does not require special protective clothing and does not harm human health. Children are also not at risk if they accidentally ingest the product.
“Most farmers have small farms – quarter acre, half acre, at most three acres,” said Makokha. “For a quarter acre you spend five dollars and you get more yields. Two of them would be approximately five dollars – that’s enough for a whole season – so it is pocket friendly.”
And if the company is able to harvest the material in Kenya, it would be even cheaper.
“You can imagine if we dredge here – probably (get the cost down to) a dollar – so it makes more sense for the farmers.”
The dredging has another positive impact: it helps with managing flooding by making the lake deeper once the silt is dredged out, making life better and safer for people living nearby.
BioDeposit has been operating in Kenya for a year and, Makokha said, “the response is awesome.”
BioDeposit organizes workshops for farmers through cooperative societies, helping to guide farmers through the whole process of becoming organically certified.
The company believes its products will help avert problems such as what happened recently when the European Union prevented some flowers – a major source of overseas income for Kenyan farmers – from entering the EU because of banned pesticides.
Cleverly, BioDeposit does most of its business digitally through mobile phones. It conducts its business with sales representatives by phone and conducts training by phone as well. All payments and bank transfers are done by phone using the M-PESA system (http://www.safaricom.co.ke/?id=257).
“It is the easiest way to do business in Kenya,” said Makokha. “Everybody right now owns a mobile phone. When we get the M-PESA, we transfer directly to the account. You get the money and transfer to the bank account and you are done, very easy for everybody … doing wonders for us.”
By David South, Development Challenges, South-South Solutions
Published: March 2014
Development Challenges, South-South Solutions was launched as an e-newsletter in 2006 by UNDP's South-South Cooperation Unit (now the United Nations Office for South-South Cooperation) based in New York, USA. It led on profiling the rise of the global South as an economic powerhouse and was one of the first regular publications to champion the global South's innovators, entrepreneurs, and pioneers. It tracked the key trends that are now so profoundly reshaping how development is seen and done. This includes the rapid take-up of mobile phones and information technology in the global South (as profiled in the first issue of magazine Southern Innovator), the move to becoming a majority urban world, a growing global innovator culture, and the plethora of solutions being developed in the global South to tackle its problems and improve living conditions and boost human development. The success of the e-newsletter led to the launch of the magazine Southern Innovator.
Follow @SouthSouth1
Google Books: https://books.google.co.uk/books?id=WBM9BQAAQBAJ&dq=development+challenges+march+2014&source=gbs_navlinks_s
Slideshare: http://www.slideshare.net/DavidSouth1/development-challenges-march-2014-published-44135069
Southern Innovator Issue 1: https://books.google.co.uk/books?id=Q1O54YSE2BgC&dq=southern+innovator&source=gbs_navlinks_s
Southern Innovator Issue 2: https://books.google.co.uk/books?id=Ty0N969dcssC&dq=southern+innovator&source=gbs_navlinks_s
Southern Innovator Issue 3: https://books.google.co.uk/books?id=AQNt4YmhZagC&dq=southern+innovator&source=gbs_navlinks_s
Southern Innovator Issue 4: https://books.google.co.uk/books?id=9T_n2tA7l4EC&dq=southern+innovator&source=gbs_navlinks_s
Southern Innovator Issue 5: https://books.google.co.uk/books?id=6ILdAgAAQBAJ&dq=southern+innovator&source=gbs_navlinks_s
 The first five issues of Southern Innovator. The highly influential magazine was distributed around the world and each issue was launched at the annual Global South-South Development (GSSD) Expo hosted by the United Nations Office for South-South Cooperation (UNOSSC).
The first five issues of Southern Innovator. The highly influential magazine was distributed around the world and each issue was launched at the annual Global South-South Development (GSSD) Expo hosted by the United Nations Office for South-South Cooperation (UNOSSC).
This work is licensed under a
Creative Commons Attribution-Noncommercial-No Derivative Works 3.0 License.
Agribusiness, Development Challenges, South-South Solutions, Global South-South Development Expo, Solutions, Southern Innovator Magazine, UN Innovator Stories, UNDP, UNDP Innovator Stories, UNOSSC, United Nations